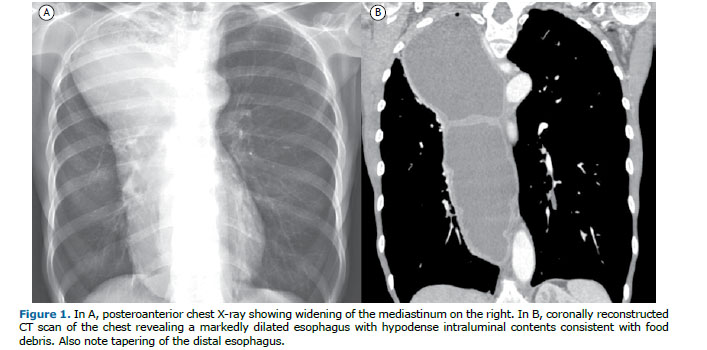
A 68-year-old man presented with a 1-year history of progressive dysphagia, retrosternal discomfort, and 6-month history of weight loss (10 kg). A chest X-ray showed widening of the mediastinum on the right (Figure 1A).
A chest X-ray and a chest CT scan (Figure 1) showed that the widening of the mediastinum corresponded to a markedly dilated esophagus containing fluid, consistent with megaesophagus. Conceptually, megaesophagus represents dilatation of the esophagus due to several causes, such as achalasia, tumors, and connective tissue diseases.
On imaging (chest X-ray, esophagography, and chest CT), the classic megaesophagus appears as widening of the mediastinum, being characterized by a vertical soft-tissue density, usually with thin walls and heterogeneous contents consisting of food debris. It often contains an air-fluid level and is distally tapered (bird’s beak appearance).
Achalasia is a primary esophageal motility disorder characterized by a lack of esophageal peristalsis and partial or absent relaxation of the lower esophageal sphincter, making it difficult for the bolus to pass. Achalasia can be divided into primary (idiopathic), which is the most common form worldwide, or secondary. The major secondary cause of achalasia in Brazil is Chagas disease (CD).(1-3)
CD, also known as American trypanosomiasis, is caused by the protozoan Trypanosoma cruzi, which is highly prevalent and causes significant morbidity in Latin America. Currently, an extremely high number of patients still suffer from this disease, most of whom are elderly. In CD-endemic areas, it is essential that the possibility of esophageal disease caused by CD be considered in patients with megaesophagus.(1-3) Our patient has had a confirmed diagnosis of CD for approximately 16 years.
CD can present in two forms: acute or chronic. The chronic form of CD develops a few decades after the initial infection, causing irreversible damage to the heart, esophagus (megaesophagus), and colon (megacolon). The symptoms of and morphological changes in the digestive tract are due to impairment of neurons and nerve ganglia. The most common symptom is dysphagia, followed by regurgitation, a feeling of fullness when eating or drinking, heartburn, and chest pain. Dysphagia runs a chronic course, lasting for several years, and is progressive. Patients with CD-associated megacolon experience severe prolonged constipation for years or decades. A final diagnosis of chronic CD is based on serological tests. Surgery is currently the best form of treatment.(1-3)
REFERENCES 1. Marchiori E. Chagas disease: a tropical infection of interest to the radiologist. Radiol Bras. 2016;49(6):V-VI. https://doi.org/10.1590/0100-3984.2016.49.6e1
2. Abud TG, Abud LG, Vilar VS, Szejnfeld D, Reibscheid S. Radiological findings in megaesophagus secondary to Chagas disease: chest X-ray and esophagogram. Radiol Bras. 2016;49(6):358-362. https://doi.org/10.1590/0100-3984.2015.0141
3. Schlottmann F, Patti MG. Esophageal achalasia: current diagnosis and treatment. Ex-pert Rev Gastroenterol Hepatol. 2018;12(7):711-721. https://doi.org/10.1080/17474124.2018.1481748






 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket




