ABSTRACT
Objective: To determine the characteristics of individuals with asthma who are responsive to aerobic training. Methods: This post hoc analysis of pooled data from previous randomized controlled trials involved 101 individuals with moderate to severe asthma who underwent aerobic training. Participants underwent a maximal cardiopulmonary exercise test and completed the Asthma Control Questionnaire and the Asthma Quality of Life Questionnaire before and after a 24-session aerobic training program. Better and worse responders to aerobic training were identified by cluster analysis. Results: Two clusters were identified according to the improvement in peak VO2 after aerobic training (better and worse responders). Characteristics of the better responder group were being older, being female, having higher BMI, and having higher cardiac reserve at baseline when compared with the worse responder group. Also, better responders had worse clinical control, worse quality of life, and lower physical capacity at baseline. After training, worse responders, in comparison with better responders, showed half the improvement in ?peak VO2 (7.4% vs. 13.6%; 95% CI, -12.1 to -0.92%; p < 0.05) and worse asthma control. A weak, negative, but significant association (r = -0.35; p < 0.05) was observed between clinical control and aerobic fitness only in the better responder group. Both groups showed significant improvement in quality of life. Conclusions: Obese individuals with worse exercise capacity, clinical control, and quality of life showed improvement with aerobic training. Moreover, worse responders also improved with training, but to a lesser extent.
Keywords:
Asthma; Exercise therapy; Cluster analysis; Status Asthmaticus; Quality of Life; Rehabilitation.
RESUMO
Objetivo: Determinar as características de indivíduos com asma responsivos a treinamento aeróbio. Métodos: Esta análise post hoc de dados agrupados provenientes de ensaios clínicos controlados randomizados anteriores envolveu 101 indivíduos com asma moderada a grave submetidos a treinamento aeróbico. Os participantes foram submetidos a um teste de exercício cardiopulmonar máximo e responderam ao Asthma Control Questionnaire e ao Asthma Quality of Life Questionnaire antes e depois de um programa de treinamento aeróbio de 24 sessões. Melhores e piores respondedores ao treinamento aeróbio foram identificados por análise de conglomerados. Resultados: Foram identificados dois conglomerados de acordo com a melhora do VO2 de pico após o treinamento aeróbio (melhores e piores respondedores). As características do grupo melhor respondedor foram maior idade, sexo feminino, IMC mais elevado e maior reserva cardíaca basal em comparação com o grupo pior respondedor. Os melhores respondedores também apresentavam pior controle clínico, pior qualidade de vida e menor capacidade física basal. Após o treinamento, os piores respondedores, em comparação com os melhores respondedores, apresentaram metade da melhora no ΔVO2 de pico (7,4% vs. 13,6%; IC95%: -12,1 a -0,92%; p < 0,05) e pior controle da asma. Observou-se uma associação negativa fraca, mas significativa (r = −0,35; p < 0,05) entre controle clínico e aptidão aeróbia apenas no grupo melhor respondedor. Ambos os grupos apresentaram melhora significativa da qualidade de vida. Conclusões: Os indivíduos obesos com pior capacidade de exercício, controle clínico e qualidade de vida apresentaram melhora com o treinamento aeróbio. Além disso, os piores respondedores também melhoraram com o treinamento, mas em menor grau.
Palavras-chave:
Asma; Terapia por exercício; Análise por conglomerados; Estado asmático; Qualidade de vida; Reabilitação.
INTRODUCTION Asthma is defined as a heterogeneous disease, usually characterized by chronic airway inflammation.(1) Asthma leads to systemic inflammation, exercise-induced bronchospasm, and development of comorbidities. In addition, this condition promotes increased levels of anxiety and depression and reduced physical activity levels, leading to a reduction in the physical capacity of these individuals.(2) However, the increase in exercise capacity by means of physical training at moderate intensity in individuals with asthma improves immune responses and reduces airway inflammation.(3) Exercise also decreases exercise-induced bronchoconstriction(3) and corticosteroid use.(4) In addition, physical training in individuals with moderate to severe asthma improves clinical asthma control(5,6) and health factors related to the individual’s quality of life(3,7); conversely, the association between physical fitness and clinical control is still poorly understood.
It remains unknown who would most benefit from a physical training program(8) and whether there would be a certain subgroup of individuals who do not respond to a specific training program.(9) Pulmonary rehabilitation is an expensive and time-consuming program. Ambrosino and Clini(10) stated the importance of knowing the predictors of a successful pulmonary rehabilitation program in individuals with COPD to optimize the use of financial resources in this field. The response to a pulmonary rehabilitation program is multidimensional.(11) For example, COPD responders to pulmonary rehabilitation presented with more severe dyspnea symptoms, greater number of hospitalizations, more severe anxiety and depression symptoms, greater BMI, worse health condition, and worse exercise performance prior to the intervention. (11) Another study demonstrated that obese individuals with COPD with better lung function and worse physical activity levels at baseline benefited more from a pulmonary rehabilitation program.(12)
Despite the well-known benefits of improving exercise capacity in individuals with asthma, the factors determining those who respond to a pulmonary rehabilitation program have been exclusively reported in individuals with COPD. Although these factors could be obvious and may be applied to other chronic pulmonary diseases, determining these factors is mandatory due to the specific characteristics and impact on the lives of patients with asthma. So far, there is no information on which individuals with asthma respond to aerobic training or pulmonary rehabilitation programs. Therefore, this study aimed to determine the characteristics of individuals with moderate to severe asthma who respond to aerobic training and the relationship between that response with changes in clinical control, quality of life, and exercise capacity.
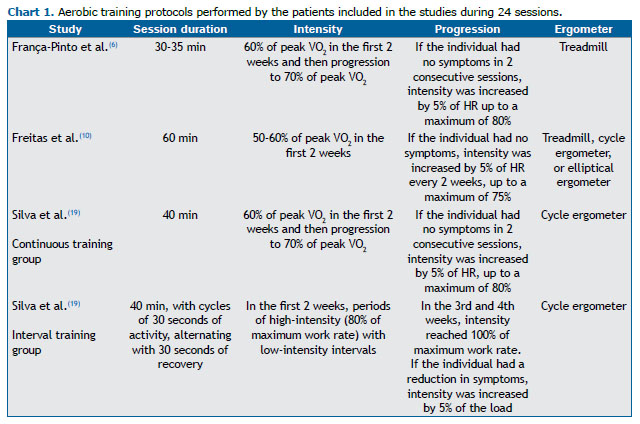
METHODS This was a post hoc analysis of pooled data from previous randomized controlled trials.(3,6,13) These trials involved individuals with moderate to severe asthma who had previously participated in a pulmonary rehabilitation program in our center and underwent aerobic training (Chart 1).(3,6,13) There was no overlap of individuals among the studies. All individuals were followed at the same university hospital. The research ethics committee of the institution approved the clinical studies (CAAE no. 0121/10; no. 07137512.9.0000.0068; and no. 18178013.9.0000.0068).(3,6,13) All of the participants completed the aerobic training program between 2015 and 2019. Cardiopulmonary exercise test (CPET) variables, asthma clinical control, and quality of life were evaluated before and after the intervention.
Individuals aged 20-60 years and with a diagnosis of asthma (severity level in accordance with the criteria established by the Global Initiative for Asthma)(1) in each of the studies, based on the level of treatment needed to control exacerbations and symptoms, were included in the present study. Individuals should have had medical follow-up for at least six months, using optimized medical treatment for asthma, and clinical stability (no need to change medications, no visits to the emergency room, and no hospitalizations within 30 days at least).
Exclusion criteria were having other chronic lung disease, cancer, cardiovascular disease, or musculoskeletal dysfunction that could interfere with the assessments and/or physical exercises. In addition, those who were pregnant, current or former smokers (≥ 10 pack-years), unable to understand the instructions given by researchers, or participating in another research protocol were also excluded.
All individuals underwent a 24-session aerobic training program. Training parameters were determined by assessing VO2 during a pre-rehabilitation CPET, and they were similar among the studies (Chart 1). Before and after the intervention, pulmonary function was assessed via spirometry,(14) and FEV1 and FVC were analyzed using the predicted values for the Brazilian population.(15) Clinical control was assessed using the Brazilian-Portuguese version of the 7-item Asthma Control Questionnaire (ACQ-7).(16) The questions on the ACQ-7 are related to symptoms, activity limitations, dyspnea, wheezing, and use of rescue bronchodilators in the last week.(16) The last item on the ACQ-7 refers to a question that assesses FEV1 (in % of the predicted value, pre-bronchodilator). This questionnaire contains seven items on a 7-point scale (0 = no limitation and 6 = maximum limitation). Higher scores indicate worse clinical control. A score of 1.5 or greater is considered uncontrolled asthma.(17) A change of 0.5 point in the ACQ-7 score is considered clinically effective.(18) In addition, the health-related quality of life in asthma was assessed by the Brazilian-Portuguese version of the Asthma Quality of Life Questionnaire (AQLQ).(19) The AQLQ contains 32 items and is divided into four domains: activity limitations, symptoms, emotional function, and environmental exposure. Higher scores indicate better quality of life. A change of 0.5 point in the AQLQ score is considered clinically effective.(20)
Exercise capacity was assessed via a maximal CPET to the limits of tolerance performed either on a treadmill(3) or on a cycle ergometer.(6,13) The protocols used were previously established for treadmill(21,22) and cycle ergometer.(23) The comparison between predicted VO2max values obtained on two ergometers was corrected according to the equation(24):
VO2max = 45.2 − 0.35 × age − 10.9 × sex − 0.15 × weight + 0.68 × height − 0.46 × exercise mode
where VO2max is in mL·kg–1·min–1; age, in years; sex (male = 1; female = 2); weight, in lb; height, in inches; and exercise mode (treadmill = 1; cycle ergometer = 2). That was required due to the difference between the energy expenditure assessed on the two ergometers. (25) The CPET variables were VO2 at baseline, in mL/min; anaerobic threshold (AT), in mL·kg–1·min–1; and peak exercise, in % predicted.(24) In addition, Ve, maximum HR, and respiratory exchange ratio (RER) were recorded at the end of the test.
Data were analyzed for normality using the Kolmogorov-Smirnov test. Cluster analysis was performed in two steps.(26) Initially, a hierarchical analysis using Ward’s method automatically determined the number of clusters. Subsequently, the k-means algorithm analysis was used to group the individuals into the clusters. Cluster analysis was performed including the following variables: age; FEV1 (% predicted); BMI; pre-intervention VO2AT; pre-intervention peak VO2; (post/pre-intervention) ΔAQLQ score; (post/pre-intervention) ΔACQ-7 score; and post/pre test Δpeak VO2. The t-test was used to compare the clusters. The z-test was used to compare proportions between the clusters. Pearson’s tests were used to analyze the correlation between ΔVO2 and ΔACQ-7 in both clusters. The Statistical Package for the Social Sciences, version 12.0 (SPSS Inc., Chicago, IL, USA) and the SigmaStat software, version 3.5 (Systat Software Inc., Chicago, IL, USA) were used. The significance level was set al 5% (p < 0.05).
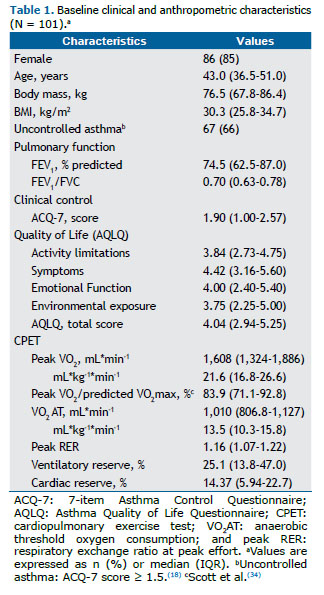
RESULTS This study involved 101 individuals with asthma who completed an aerobic training program: 22 from the study by França-Pinto et al.,(3) 26 from the study by Freitas et al.,(6) and 53 from the study by Aparecido da Silva et al.,(13) allocated in two groups: interval training group and continuous training group.
Among all of the individuals included, 55 (54.5%) were obese (BMI > 30 kg/m2), 49 (48.5%) presented with moderate airway obstruction (Table 1), and 67 (66.3%) had uncontrolled asthma. Regarding the response to maximum CPET, 32 (31.7%) of the individuals presented limitations in the ventilatory system, as did 51 (50.5%) in the cardiovascular system and 65 (64.4%) in the peripheral muscle system.
After cluster analysis, the two groups were determined based on the improvement in peak VO2 after aerobic training. The groups were classified as better or worse responders to aerobic training (Table 2). Before the intervention, the better responder group mostly consisted of females and older individuals with higher BMI and higher cardiac reserve in comparison with the worse responder group. In addition, the better responder group presented with worse clinical control and worse quality of life before training and lower physical capacity (peak VO2 and VO2AT) than did the worse responder group. In contrast, pulmonary function (FEV1 and FEV1/FVC ratio) and ventilatory reserve were similar between the groups. After the training program, the better responder group showed twice the improvement in Δpeak VO2 when compared with the worse responder group. Only the better responder group showed a clinically significant improvement on clinical asthma control (a decrease ≥ 0.5 in the ACQ-7 score), which was associated with aerobic power improvement (Figure 1).


Both groups had a clinically significant improvement in health-related quality of life (an increase ≥ 0.5 in AQLQ score) after the intervention (Table 2). Cardiac and respiratory reserves, VO2AT, and peak VO2 after the CPET were similar between the groups.
DISCUSSION Our results showed the characteristics of individuals with moderate to severe asthma who significantly responded to aerobic training. Females and older individuals with a higher BMI, as well as with worse aerobic capacity, clinical control, and quality of life, had a good response to aerobic training. Although these results seem intuitive, this is the first study to investigate such clinical characteristics. In addition, it was observed that both groups showed clinically significant improvement in health aspects related to quality of life.
Several systematic reviews have investigated the benefits of physical exercise in improving exercise capacity, quality of life, and symptoms in individuals with asthma.(27-29) However, limited information regarding which individuals with asthma benefit more from aerobic training is available. In this study, there was a predominance of females in the better responder group, and two explanations can support this finding. First, there is a higher prevalence of adult females with moderate to severe asthma.(30) Second, middle-aged females tend to be more sedentary, to be overweight/obese, and to present worse physical conditioning even when they do not have asthma.(31,32) This may also explain the differences in age between the groups. However, we do not believe that our results establish a priority for physical training in female individuals with asthma. Instead, the priority should be on individuals having low physical conditioning, obesity, and clinically uncontrolled disease.
Previous studies reported that nonobese individuals with controlled asthma(3,5) and obese individuals with uncontrolled asthma(6) improve their aerobic conditioning and quality of life after a physical training program. These findings support our results, because we found no differences regarding quality of life between the groups after a physical training program. However, the better responder group showed twice the improvement in aerobic capacity (Δpeak VO2) than did the worse responder group. This improvement cannot be associated with differences among the training programs, because exercise intensity was similarly established based on a CPET in all studies, regardless of the training modality (continuous or interval training).(13) Likewise, we believe that using a treadmill for half of the sample instead of a cycle ergometer did not interfere with the results since all of the participants improved their aerobic capacity. Our results indicated that individuals with moderate to severe asthma with low AT and aerobic power had a greater increase in their physical conditioning after aerobic training.
Individuals with uncontrolled asthma before training mostly benefit from controlling asthma symptoms and present a clinically significant change (> 0.5 point in ACQ-7).(5,6,17) Obesity and poor clinical control of asthma have been associated with worse physical conditioning(30); therefore, it is more common to identify individuals who have more than one factor associated with exercise response. We consider that aerobic training prescription for individuals with asthma should be recommended for those who have poor asthma control, despite having optimized pharmacological treatment (inclusion criteria of all patients in the present study). In addition, our results support that the benefits of exercise training should be analyzed differently in individuals with and without asthma control in future studies. This approach may improve our understanding of the effects of physical training in this population.
Three theories have been suggested to explain how the improvement in aerobic capacity in individuals with asthma reduces symptoms and improves asthma control: improvement in ventilatory capacity,(27) improvement in pulmonary function,(28) and reduction in pulmonary and systemic inflammation.(3,6) Our results showed that individuals with asthma had reduced ventilatory reserve at baseline (25% on average) in comparison with the general population (approximately 50%) and close to the cutoff value to establish a ventilatory limitation (< 20%).(23) Furthermore, we observed that individuals with asthma had reduced aerobic capacity and cardiac reserve, strongly suggesting that they were physically unfit before exercise training. Thus, our results reinforce that exercise training improves aerobic fitness in individuals with asthma, demanding an increase in ventilatory capacity.
In this study, only the better responder group showed a linear association between improvements in physical conditioning and clinical control. A possible explanation for this association is that improving aerobic fitness improves aerobic capacity, reduces ventilation in activities of daily living, and reduces asthma symptoms. Previous randomized and controlled studies also suggested that training improves immune response,(3,6) but a systematic review suggested that there was no effect in the immune response of asthma patients.(28) However, that review included patients with different levels of asthma severity and clinical control that might have interfered with data analysis. Furthermore, not all individuals included in our study were evaluated for pulmonary and systemic inflammation, making this type of analysis impossible.
Before training, individuals in both groups showed lower AQLQ scores in our study than in previous studies. (5,7,33,34) Better responders to aerobic training had AQLQ scores even lower than did worse responders. After training, both groups showed clinically significant improvement, and previous studies support our findings. (5,7,33,34) There was no association between improved aerobic power and quality of life. One hypothesis for this finding would be the multifactorial aspect of quality of life. The AQLQ has several domains (activity limitations, symptoms, emotional function, and environmental exposure) that can be modified by exercise training, regardless of the physical conditioning obtained by each individual.(20)
This study has limitations. First, this was a post hoc analysis of pooled data from previous randomized controlled trials, not a prospective study. However, this limitation is mitigated by the number of patients and variables evaluated, and all individuals underwent physical training in the same research center using similar exercise intensity. Furthermore, we believe no other center has such a large number of individuals undergoing physical training, based on CPET results, being assessed regarding asthma clinical control and quality of life. Second, most individuals in this study were females; however, this was expected due to the higher prevalence of asthma in female individuals, and the fact that females seek medical care more regularly than do males.(30) Furthermore, females with asthma have a high prevalence of obesity and uncontrolled asthma. However, our female patients had a wide distribution of obese and nonobese individuals with controlled and uncontrolled asthma. Third, the effect on inflammatory mediators was not included, because only two studies assessed this outcome,(6,13) making it impossible to include it in the statistical analyses. Additionally, muscle strength could be associated with a patient’s response to the physical training program, and the improvement in peripheral muscle response could also add important information; however, this variable was not evaluated by any of the studies herein included. Finally, exercise limitation was categorized as cardiac, ventilatory, and peripheral muscle systems, which can be considered a simplified way to understand individual limitations of the patients. However, this analysis has been considered in individuals with asthma(35) and in other populations.(23) In addition, we did not use these physiological responses to determine the main reason by which patients would necessarily interrupt the test. Instead, this analysis was secondarily used to understand the major limitation in each cluster.
The results of this study show that obese individuals with poor exercise capacity, clinical control, and quality of life obtained greater benefits from an aerobic training program. Therefore, individuals with these characteristics should be primarily referred to aerobic training programs in order to reduce asthma symptoms. Better and worse responders to aerobic training had similar improvements in their quality of life.
AUTHOR CONTRIBUTIONS TCE, ACL, PDF, and CRFC: study conception and design. TCE and ACL: data analysis and drafting of the manuscript. PDF, RAS, FARM, and AFP: data collection and critical revision of the manuscript. RMCP and CRFC: critical and final revision of the manuscript. All authors approved the final manuscript.
CONFLICTS OF INTEREST The authors declare that the results of the study are presented clearly, honestly, and without fabrication, falsification, or inappropriate data manipulation.
The authors declare they have no conflicts of interest to disclose.
DATA AVAILABILITY STATEMENT The database is available in the repository: https://zenodo.org/record/6326209#.YyospqTMK5c
REFERENCES 1. Global Initiative for Asthma (GINA) [homepage on the Internet]. Bethesda: GINA; c2021 [cited 2021 Jul 1]. Global Strategy for Asthma Management and Prevention (Updated 2021). [Adobe Acrobat document, 217p.]. Available from: https://ginasthma.org/wp content/uploads/2021/05/GINA Main Report 2021 V2 WMS.pdf
2. Carvalho Pinto RM, Cançado JED, Pizzichini MMM, Fiterman J, Rubin AS, Cerci Neto A, et al. 2021 Brazilian Thoracic Association recommendations for the management of severe asthma. J Bras Pneumol. 2021;47(6):e20210173. https://doi.org/10.36416/1806-3756/e20210273
3. França-Pinto A, Mendes FA, de Carvalho-Pinto RM, Agondi RC, Cukier A, Stelmach R, et al. Aerobic training decreases bronchial hyperresponsiveness and systemic inflammation in patients with moderate or severe asthma: a randomised controlled trial. Thorax. 2015;70(8):732-739. https://doi.org/10.1136/thoraxjnl-2014-206070
4. Neder JA, Nery LE, Silva AC, Cabral AL, Fernandes AL. Short-term effects of aerobic training in the clinical management of moderate to severe asthma in children. Thorax. 1999;54(3):202-206. https://doi.org/10.1136/thx.54.3.202
5. Dogra S, Kuk JL, Baker J, Jamnik V. Exercise is associated with improved asthma control in adults. Eur Respir J. 2011;37(2):318-323. https://doi.org/10.1183/09031936.00182209
6. Freitas PD, Ferreira PG, Silva AG, Stelmach R, Carvalho-Pinto RM, Fernandes FL, et al. The Role of Exercise in a Weight-Loss Program on Clinical Control in Obese Adults with Asthma. A Randomized Controlled Trial. Am J Respir Crit Care Med. 2017;195(1):32-42. https://doi.org/10.1164/rccm.201603-0446OC
7. Turner S, Eastwood P, Cook A, Jenkins S. Improvements in symptoms and quality of life following exercise training in older adults with moderate/severe persistent asthma. Respiration. 2011;81(4):302-310. https://doi.org/10.1159/000315142
8. Herigstad M, Faull OK, Hayen A, Evans E, Hardinge FM, Wiech K, et al. Treating breathlessness via the brain: changes in brain activity over a course of pulmonary rehabilitation. Eur Respir J. 2017;50(3):1701029. https://doi.org/10.1183/13993003.01029-2017
9. Montero D, Lundby C. Refuting the myth of non-response to exercise training: ‘non-responders’ do respond to higher dose of training [published correction appears in J Physiol. 2018 Apr 1;596(7):1311]. J Physiol. 2017;595(11):3377-3387. https://doi.org/10.1113/JP273480
10. Ambrosino N, Clini EM. Response to pulmonary rehabilitation: toward personalised programmes?. Eur Respir J. 2015;46(6):1538-1540. https://doi.org/10.1183/13993003.01125-2015
11. Spruit MA, Augustin IM, Vanfleteren LE, Janssen DJ, Gaffron S, Pennings HJ, et al. Differential response to pulmonary rehabilitation in COPD: multidimensional profiling. Eur Respir J. 2015;46(6):1625-1635. https://doi.org/10.1183/13993003.00350-2015
12. Buekers J, DE Boever P, Theunis J, Houben-Wilke S, Vaes AW, Franssen FME, et al. Physiological Changes Differ between Responders and Nonresponders to Pulmonary Rehabilitation in COPD. Med Sci Sports Exerc. 2021;53(6):1125-1133. https://doi.org/10.1249/MSS.0000000000002578
13. Aparecido da Silva R, Leite Rocco PG, Stelmach R, Mara da Silva Oliveira L, Sato MN, Cukier A, et al. Constant-Load Exercise Versus High-Intensity Interval Training on Aerobic Fitness in Moderate-to-Severe Asthma: A Randomized Controlled Trial. J Allergy Clin Immunol Pract. 2022;10(10):2596-2604.e7. https://doi.org/10.1016/j.jaip.2022.05.023
14. Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al; ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26(2):319-338. https://doi.org/10.1183/09031936.05.00034805
15. Pereira CA, Sato T, Rodrigues SC. New reference values for forced spirometry in white adults in Brazil. J Bras Pneumol. 2007;33(4):397-406. https://doi.org/10.1590/S1806-37132007000400008
16. Leite M, Ponte EV, Petroni J, D’Oliveira Júnior A, Pizzichini E, Cruz AA. Evaluation of the asthma control questionnaire validated for use in Brazil. J Bras Pneumol. 2008;34(10):756-763. https://doi.org/10.1590/S1806-37132008001000002
17. Juniper EF, Bousquet J, Abetz L, Bateman ED; GOAL Committee. Identifying ‘well-controlled’ and ‘not well-controlled’ asthma using the Asthma Control Questionnaire. Respir Med. 2006;100(4):616-621. https://doi.org/10.1016/j.rmed.2005.08.012
18. Juniper EF, Svensson K, Mörk AC, Ståhl E. Measurement properties and interpretation of three shortened versions of the asthma control questionnaire. Respir Med. 2005;99(5):553-558. https://doi.org/10.1016/j.rmed.2004.10.008
19. De Oliveira MA, Barbiere A, Santos LA, Faresin SM, Fernandes AL. Validation of a simplified quality-of-life questionnaire for socioeconomically deprived asthma patients. J Asthma. 2005;42(1):41-44. https://doi.org/10.1081/JAS-200044772
20. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a minimal important change in a disease-specific Quality of Life Questionnaire. J Clin Epidemiol. 1994;47(1):81-87. https://doi.org/10.1016/0895-4356(94)90036-1
21. Heyward VH. Advanced fitness assessment and exercise prescription. Champaign, IL: Human Kinetics; 1997. p. 322.
22. Santos-Silva PR, Fonseca AJ, Castro AW, Greve JM, Hernandez AJ. Reproducibility of maximum aerobic power (VO2max) among soccer players using a modified heck protocol. Clinics (Sao Paulo). 2007;62(4):391-396. https://doi.org/10.1590/S1807-59322007000400004
23. Wasserman K, Hansen JE, Sue DY, Casaburi R, Whipp BJ. Pathophysiology of disorders limiting exercise. In: Principles of Exercise Testing and Interpretation. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 1999. p. 1142-1195.
24. de Souza E Silva CG, Kaminsky LA, Arena R, Christle JW, Araújo CGS, Lima RM, et al. A reference equation for maximal aerobic power for treadmill and cycle ergometer exercise testing: Analysis from the FRIEND registry. Eur J Prev Cardiol. 2018;25(7):742-750. https://doi.org/10.1177/2047487318763958
25. American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing [published correction appears in Am J Respir Crit Care Med. 2003 May 15;1451-2]. Am J Respir Crit Care Med. 2003;167(2):211-277. https://doi.org/10.1164/rccm.167.2.211
26. Cluster analysis. In: Mooi E, Sarstedt M. A Concise Guide to Market Research. Berlin, Heidelberg: Springer-Verlag; 2011. p. 237-284. https://doi.org/10.1007/978-3-642-12541-6_9
27. Ram FS, Robinson SM, Black PN. Effects of physical training in asthma: a systematic review. Br J Sports Med. 2000;34(3):162-167. https://doi.org/10.1136/bjsm.34.3.162
28. Hansen ESH, Pitzner-Fabricius A, Toennesen LL, Rasmusen HK, Hostrup M, Hellsten Y, et al. Effect of aerobic exercise training on asthma in adults: a systematic review and meta-analysis. Eur Respir J. 2020;56(1):2000146. https://doi.org/10.1183/13993003.00146-2020
29. Kuder MM, Clark M, Cooley C, Prieto-Centurion V, Danley A, Riley I, Siddiqi A, et al. A Systematic Review of the Effect of Physical Activity on Asthma Outcomes. J Allergy Clin Immunol Pract. 2021;9(9):3407-3421.e8. https://doi.org/10.1016/j.jaip.2021.04.048
30. de Carvalho-Pinto RM, Cukier A, Angelini L, Antonangelo L, Mauad T, Dolhnikoff M, et al. Clinical characteristics and possible phenotypes of an adult severe asthma population. Respir Med. 2012;106(1):47-56. https://doi.org/10.1016/j.rmed.2011.08.013
31. Ribeiro MA, Martins MA, Carvalho CR. Interventions to increase physical activity in middle-age women at the workplace: a randomized controlled trial. Med Sci Sports Exerc. 2014;46(5):1008-1015. https://doi.org/10.1249/MSS.0000000000000190
32. Freitas PD, Xavier RF, McDonald VM, Gibson PG, Cordova-Rivera L, Furlanetto KC, et al. Identification of asthma phenotypes based on extrapulmonary treatable traits. Eur Respir J. 2021;57(1):2000240. https://doi.org/10.1183/13993003.00240-2020
33. Pakhale S, Baron J, Dent R, Vandemheen K, Aaron SD. Effects of weight loss on airway responsiveness in obese adults with asthma: does weight loss lead to reversibility of asthma?. Chest. 2015;147(6):1582-1590. https://doi.org/10.1378/chest.14-3105
34. Scott HA, Gibson PG, Garg ML, Pretto JJ, Morgan PJ, Callister R, et al. Dietary restriction and exercise improve airway inflammation and clinical outcomes in overweight and obese asthma: a randomized trial. Clin Exp Allergy. 2013;43(1):36-49. https://doi.org/10.1111/cea.12004
35. Ferreira PG, Freitas PD, Silva AG, Porras DC, Stelmach R, Cukier A, et al. Dynamic hyperinflation and exercise limitations in obese asthmatic women. J Appl Physiol (1985). 2017;123(3):585-593. https://doi.org/10.1152/japplphysiol.00655.2016












 Read in Portuguese
Read in Portuguese
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket