ABSTRACT
Objective: To evaluate the efficacy of wearing a mask to prevent COVID-19 infection. Methods: This was a systematic review and meta-analysis of cohort and case-control studies, considering the best level of evidence available. Electronic databases (MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials, and Clinical Trials.gov) were searched to identify studies that evaluated the effectiveness of wearing masks compared with that of not wearing them during the COVID-19 pandemic. Risk of bias and quality of evidence were assessed using the Cochrane risk of bias tool and the Grading of Recommendations Assessment, Development, and Evaluation. Results: Of the 1,028 studies identified, 9 met the inclusion criteria (2 cohort studies and 7 case-control studies) and were included in the analysis. The meta-analysis using cohort studies alone showed statistically significant differences, wearing a cloth mask decreased by 21% [RD = -0.21 (95% CI, -0.34 to -0.07); I2 = 0%; p = 0,002] the risk of COVID-19 infection, but the quality of evidence was low. Regarding case-control studies, wearing a surgical mask reduced the chance of COVID-19 infection [OR = 0.51 (95% CI, 0.37-0.70); I2 = 47%; p = 0.0001], as did wearing an N95 respirator mask [OR = 0.31 (95% CI, 0.20-0.49); I2 = 0%; p = 0.00001], both with low quality of evidence. Conclusions: In this systematic review with meta-analysis, we showed the effectiveness of wearing masks in the prevention of SARS-CoV-2 infection regardless of the type of mask (disposable surgical mask, common masks, including cloth masks, or N95 respirators), although the studies evaluated presented with low quality of evidence and important biases.
Keywords:
Antiviral agents; COVID-19; SARS-CoV-2; Masks.
RESUMO
Objetivo: Avaliar a eficácia do uso de máscaras na prevenção da infecção por COVID-19. Métodos: Revisão sistemática e meta-análise de estudos de coorte e caso-controle, considerando o melhor nível de evidência disponível. Bancos de dados eletrônicos (MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials e ClinicalTrials.gov) foram pesquisados para identificar estudos que avaliassem a eficácia do uso de máscaras em comparação com ausência de seu uso durante a pandemia de COVID-19. O risco de viés e a qualidade da evidência foram avaliados usando a ferramenta Cochrane risk of bias e Grading of Recommendations Assessment, Development, and Evaluation. Resultados: Dos 1.028 estudos identificados, 9 preencheram os critérios de inclusão (2 estudos de coorte e 7 estudos de caso-controle) e foram incluídos na análise. A meta-análise usando apenas estudos de coorte mostrou diferenças estatisticamente significativas: o uso de máscara de tecido diminuiu 21% [(risk difference = −0,21 (IC 95%: −0,34 a −0,07); I2 = 0%; p = 0,002] o risco de infecção por COVID-19, mas a qualidade da evidência foi baixa. Em relação aos estudos caso-controle, o uso de máscara cirúrgica reduziu a chance de infecção por COVID-19 [OR = 0,51 (IC 95%: 0,37-0,70); I2 = 47%; p = 0,0001], assim como o uso de máscara respiratória N95 [OR = 0,31 (IC 95%: 0,20-0,49); I2 = 0%; p = 0,00001], ambos com baixa qualidade de evidência. Conclusões: Nesta revisão sistemática com meta-análise, demonstramos a eficácia do uso de máscaras na prevenção da infecção por SARS-CoV-2 independentemente do tipo de máscara (máscara cirúrgica descartável, máscaras comuns, incluindo máscaras de tecido, ou respiradores N95), embora os estudos avaliados apresentassem evidências de baixa qualidade e vieses importantes.
Palavras-chave:
Agentes antivirais; COVID 19; SARS-CoV-2; Máscaras.
INTRODUÇÃO Após o primeiro caso de COVID-19 em novembro de 2019, a pandemia se espalhou amplamente pelo mundo, causando inúmeras mortes por SDRA relacionada ao SARS-CoV-2. A transmissão de vírus respiratórios como o SARS-CoV-2 pode ocorrer por meio de gotículas de saliva, contatos interpessoais ou superfícies contaminadas,(1,2) e pode ser evitada por barreiras e proteção por distanciamento social.
No início da pandemia, houve um aumento repentino e acentuado no consumo de equipamentos de proteção individual (EPI), que, associados ao distanciamento social, eram os únicos métodos para prevenir a propagação do vírus antes da disponibilidade da vacina. Com o advento das vacinas, houve uma redução acentuada nas taxas de infecção e mortalidade, mas essas ainda eram elevadas. Atualmente, o uso de EPI é adaptativo considerando as recomendações dos órgãos de saúde locais e as taxas de incidência de COVID-19. A OMS(3) e os U.S. Centers for Disease Control and Prevention(4) reconhecem que o uso de máscaras bem ajustadas e a manutenção do distanciamento social, como evitar ambientes lotados ou fechados, bem como limpar as mãos regularmente e cobrir espirros e tosses, reduzem a transmissão da COVID-19. As máscaras podem ser usadas para proteger pessoas saudáveis ou para prevenir a transmissão. Por outro lado, existe uma preocupação relacionada com a real eficácia dos diferentes tipos de máscaras na redução da transmissão da COVID-19. Comercialmente, existem três tipos de máscaras comumente vendidas para proteção contra contaminação aérea: máscaras faciais de tecido, usadas pela população em geral; máscaras faciais médicas (máscaras faciais cirúrgicas), usadas por agentes de saúde; e respiradores N95 ou equivalentes, usados por profissionais de saúde na presença de contaminantes aerossóis.
Revisões sistemáticas anteriores na literatura sobre o tema(5-7) não levaram em consideração a relação entre o tipo de vírus respiratório e sua taxa de infecção respiratória, o que impactou diretamente os resultados. Além disso, esses estudos tinham desenhos de estudo diferentes, criando vieses e reduzindo a qualidade e a confiabilidade dos dados obtidos. Para melhorar as informações sobre a eficácia das máscaras utilizadas durante a pandemia de COVID-19, esta revisão sistemática foi realizada com uma seleção de estudos publicados durante a pandemia, que foram estratificados de acordo com os tipos de máscaras (máscaras de tecido, máscaras cirúrgicas e respiradores N95) usados em todo o mundo, bem como os tipos de desenho do estudo.
MÉTODOS Esta revisão sistemática foi realizada de acordo com as recomendações do Preferred Reporting Items for Systematic Reviews and Meta-Analyses.(8)
Critérios de elegibilidade O protocolo deste estudo foi baseado na metodologia PICO (Pacientes de interesse, Intervenção a ser estudada, Comparação da intervenção e Resultado [Outcome] de interesse). Portanto, o enquadramento PICO no presente estudo foi o seguinte: Pacientes: adultos em risco de serem infectados pelo SARS-CoV-2; Intervenção: uso de máscaras faciais; Comparação: indivíduos que não usavam máscara; e Resultado: infecção por COVID-19. Estudos observacionais (coorte ou caso-controle) foram incluídos neste estudo e não foram impostas restrições quanto à data de publicação, idioma ou disponibilidade do texto completo.
Fontes de informação e estratégia de busca Dois autores desenvolveram uma estratégia de busca que foi revisada e aprovada pela equipe, selecionaram fontes de informação e pesquisaram sistematicamente as seguintes bases de dados: MEDLINE, EMBASE, Cochrane Central Register of Controlled Trials e ClinicalTrials.gov, bem como literatura cinzenta. A principal estratégia de busca utilizada foi a seguinte: “(mask OR masks OR N95 OR (Respiratory Protective Devices OR Respiratory Protective Device) OR face shield) AND (COVID OR COV OR CORONAVIRUS OR SARS) AND (random*) OR therapy/broad[filter] OR comparative study OR comparative studies). A estratégia de busca incluiu estudos publicados até 1º de novembro de 2022.
Seleção de estudos Dois pesquisadores independentes selecionaram e extraíram os dados dos estudos incluídos. Primeiramente, os estudos foram selecionados com base em seus títulos e resumos. Em segundo lugar, os textos completos foram avaliados para inclusão ou exclusão, e as divergências foram resolvidas por consenso ou após discussão com um terceiro pesquisador.
Coleta de dados e resultados investigados Dados referentes a autoria, ano de publicação, descrição dos pacientes, intervenções (uso de másca0ra ou controle), números absolutos de cada desfecho e período de acompanhamento foram extraídos dos estudos.
Risco de viés e qualidade da evidência O risco de viés para estudos de coorte e caso-controle foi avaliado por meio da ferramenta atual recomendada pela Cochrane Collaboration para estimar a eficácia e a segurança de estudos intervencionistas não randomizados, denominada Risk of Bias in Non-randomized Studies of Interventions.(9) Essa ferramenta avalia sete domínios de viés, classificados pelo tempo de ocorrência, assim como outros elementos fundamentais, e são expressos como de baixo risco, risco moderado, risco grave, risco crítico ou nenhuma informação.
A avaliação do risco de viés foi realizada por dois revisores independentes e, em caso de discordância, um terceiro revisor deliberou sobre a avaliação. A qualidade da evidência foi extrapolada a partir do risco de viés e foi descrita utilizando a terminologia Grading of Recommendations Assessment, Development and Evaluation(10,11) como muito baixa, baixa, moderada ou alta; a qualidade da evidência foi descrita por GRADEpro Guideline Development Tool (McMaster University, Hamilton, ON, Canadá) para meta-análises.
Síntese dos resultados e análise estatística Os desfechos categóricos foram expressos por grupo (uso de máscaras ou controle): número de eventos e risco calculado em porcentagem (dividindo o número de eventos pelo número total de indivíduos em cada grupo) para estudos de coorte e caso-controle. A eficácia do uso de máscara facial para prevenir a transmissão de infecções respiratórias por COVID-19 em ambientes comunitários foi avaliada usando ORs e seus respectivos IC95% para estudos de caso-controle. Para estudos de coorte, os efeitos das meta-análises foram relatados como risk difference (RD, diferença de risco) ou OR e IC95% correspondentes. O uso de RD mostra o tamanho do efeito absoluto na meta-análise quando comparado com o risco relativo ou o OR, e esta técnica pode ser usada quando o resultado binário é zero em ambos os braços do estudo. Utilizamos o modelo de efeito fixo ou de efeito aleatório na meta-análise para avaliar o efeito da intervenção versus controle no desfecho quando esses dados estavam disponíveis em pelo menos dois estudos. A heterogeneidade dos efeitos entre os estudos foi quantificada utilizando a estatística I2 (I2 > 50% indicando alta heterogeneidade). Para a meta-análise, foi utilizado o software Review Manager, versão 5.4 (RevMan 5; Cochrane Collaboration, Oxford, Reino Unido).(12) Os resultados foram expressos utilizando um desenho metodológico (estudo de coorte observacional).
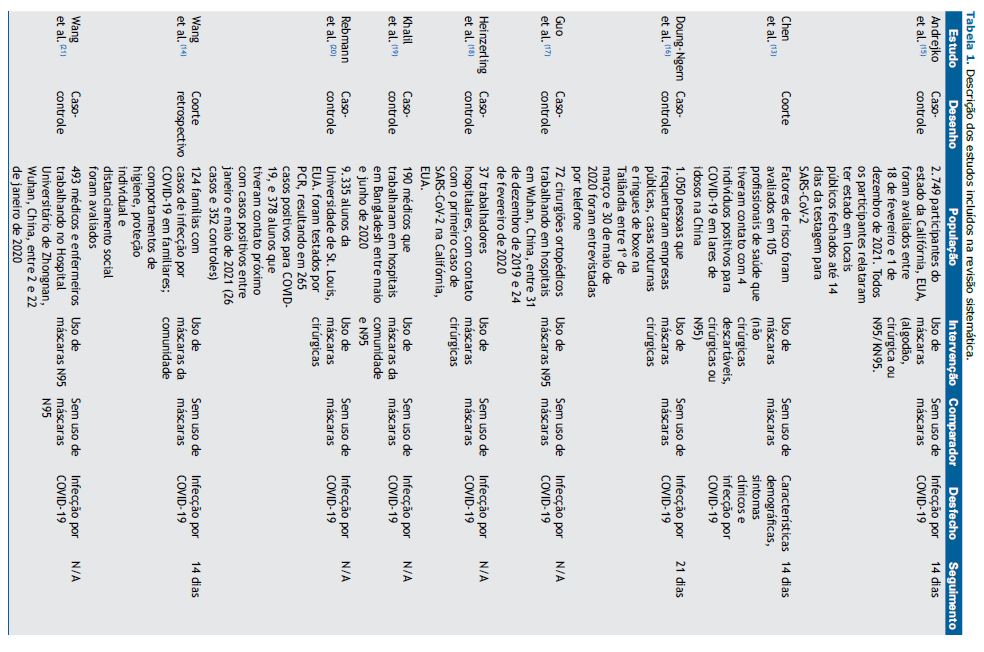
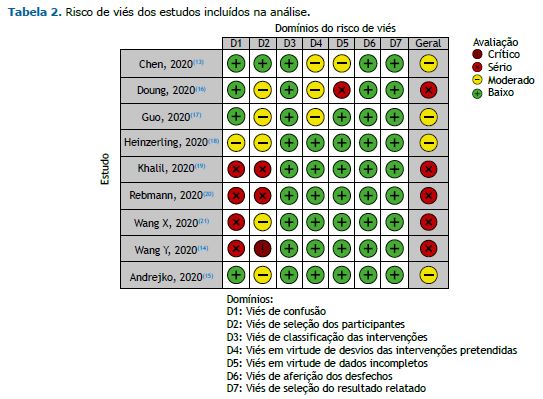
RESULTADOS Um fluxograma da busca bibliográfica e do processo de triagem é mostrado na Figura 1. A estratégia de busca identificou 1.367 estudos e, após a triagem de títulos e resumos, identificamos 57 citações potencialmente elegíveis. Após aplicação dos critérios de inclusão e exclusão, recuperamos 18 citações para análise do texto completo, e 9 estudos(13-21) foram incluídos nesta revisão sistemática, sendo 2 estudos de coorte(13,14) e 7 estudos caso-controle.(15-21) A lista de estudos excluídos e os motivos de sua exclusão estão disponíveis no material suplementar. As características dos estudos incluídos estão descritas na Tabela 1. O risco de viés e a qualidade das evidências estão descritos nas Tabelas 2 e 3, respectivamente. Nenhum viés de publicação foi identificado.
Um total de 2.803 participantes (192 nos estudos de coorte e 2.611 nos estudos de caso-controle) foi incluído na análise (uso de máscara ou não) em termos de eficácia para diminuir os índices de infecção por COVID-19.
Em relação ao risco de viés, todos os estudos incluídos apresentaram vieses altos ou críticos devido à confusão, seleção de participantes ou perda de datas. No geral, os estudos foram considerados com alto risco de viés (Tabela 2): um risco grave em 5 estudos e um risco moderado em 3 estudos.
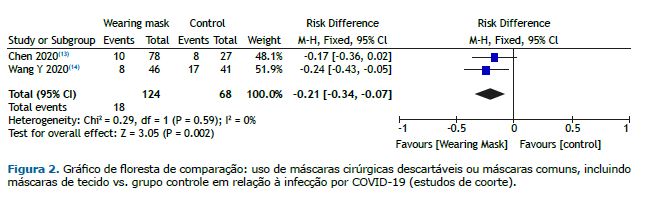
Os estudos de coorte avaliaram 192 participantes sobre a eficácia do uso de máscara (máscaras cirúrgicas descartáveis ou máscaras comuns, incluindo máscaras de tecido) na prevenção da infecção por COVID-19. O uso de máscaras foi associado a uma redução importante (em 21%) no risco de infecção por COVID-19 [RD = −0,21 (IC95%: −0,34 a −0,07); I2 = 0%; p = 0,002], indicando que era necessário que 5 participantes usassem máscaras para evitar 1 caso de COVID-19, com baixa qualidade de evidência (Figura 2).
Seis estudos caso-controle incluíram 729 indivíduos no grupo intervenção e 1.074 no grupo controle. A meta-análise mostrou que a chance de se contrair infecção por COVID-19 foi 0,49 vezes menor naqueles que usaram máscaras [OR = 0,51 (IC95%: 0,37-0,70); I2 = 47%, p = 0,0001] quando comparados com o grupo controle, com baixa qualidade de evidência (Figura 3). O uso específico das máscaras N95 foi avaliado em 4 estudos caso-controle, que incluíram 414 participantes no grupo N95 e 395 no grupo controle. O grupo N95 mostrou ter uma chance 0,69 menor de adquirir infecção por COVID-19 em comparação com aqueles que não usaram máscaras [OR = 0,31 (IC95%: 0,20-0,49); I2 = 0%, p = 0,00001], com baixa qualidade de evidência (Figura 3).
Resumo das evidências
- O uso de máscaras (máscaras cirúrgicas descartáveis ou máscaras comuns, incluindo máscaras de tecido) causou uma redução de 21% no risco de infecção por COVID-19 [RD = −0,21 (IC95%: −0,34 a −0,07); I2 = 0%, p = 0,002] nos estudos de coorte incluídos, com baixa qualidade de evidência
- O uso de máscaras cirúrgicas diminuiu a chance de infecção por COVID-19 em 49% [OR = 0,51 (IC95%: 0,37-0,70); I2 = 47%, p = 0,00001] nos estudos caso-controle incluídos, com baixa qualidade de evidência
- O uso de máscaras N95 demonstrou um efeito protetor significativo na diminuição (em 69%) da chance de infecção por COVID-19 [OR = 0,31 (IC95%: 0,20-0,49); I2 = 0%; p = 0,00001] nos estudos caso-controle incluídos, com baixa qualidade de evidência
DISCUSSÃO Nossa revisão sistemática demonstra uma redução no risco de infecção por COVID-19. Ao avaliar diferentes subgrupos de desenhos de estudo (estudos de coorte cuja intervenção foi o uso de máscaras cirúrgicas descartáveis, máscaras comuns, incluindo máscaras de tecido, ou máscaras N95; e estudos de caso-controle cuja intervenção foi o uso de máscaras cirúrgicas ou máscaras N95), obtivemos uma redução relevante no risco de infecção por COVID-19, independentemente do tipo de máscara, mas a certeza da evidência foi baixa.
Comparando os nossos resultados com os de outras revisões sistemáticas, podemos afirmar que o uso de máscaras pode contribuir para a redução da infecção por COVID-19. A literatura prévia estudou o efeito do uso de máscaras em diferentes cenários, diferentes tipos de aerossóis infecciosos e diferentes taxas de infecção. É importante promover conhecimento e educação confiáveis à sociedade sobre o uso de máscaras faciais como instrumento de proteção individual. O Japão é um dos países que educou culturalmente a sua população no uso de máscaras para proteger os outros quando apresenta sintomas respiratórios. No entanto, essa não é a única instrução que podemos fornecer para a proteção contra a infecção por COVID-19. Precisamos nos lembrar de manter o distanciamento social, a higiene das mãos e outras medidas essenciais.
Xu et al.(22) demonstraram que ambientes internos podem conter altas taxas de dispersantes de aerossóis, o que pode promover altas taxas de transmissão viral; contudo, ao usar uma máscara N95 ou uma máscara cirúrgica, o nível de aerossóis pode ser reduzido significativamente. Da mesma forma, Araújo et al.(5) demonstraram que o uso de máscaras faciais em um cenário comunitário pode diminuir significativamente as infecções virais. Além disso, as máscaras cirúrgicas oferecem maior proteção quando comparadas às máscaras de tecido. Por outro lado, para conseguir uma redução significativa na transmissão da COVID-19, mais de metade da população precisa usar máscaras. Portanto, é importante que a taxa de transmissão da infecção seja considerada pelas recomendações de saúde pública quanto ao uso de máscaras. Hoje em dia, ao observarmos uma nova cepa de SARS-CoV-2 mais transmissível, uma baixa taxa de vacinação e/ou a falta de uso de máscaras faciais podemos aguardar desfechos mais críticos, como aumentos no número de internações e mortes novamente.
Quando avaliamos o uso de máscaras sem estratificar o tipo específico de máscara ou o desenho do estudo, houve uma redução de 57% na chance de infecção por COVID-19 (Figura 3). Em relação à comparação entre máscaras cirúrgicas e N95, independente do desenho do estudo, encontramos reduções de 49% e 69% na chance de infecção por COVID-19, respectivamente. A diferença de proteção entre máscaras cirúrgicas e N95 se deve à diferença na permeabilidade do material utilizado em sua fabricação, pois o material utilizado nas máscaras N95 é menos impermeável que o utilizado nas máscaras cirúrgicas, oferecendo maior proteção. Porém, existem vieses, como tempo de uso, treinamento para uso e número de vezes de exposição a contaminantes e a locais com maior chance de contaminação, que são fatores determinantes para maior ou menor proteção na utilização de EPI.
Esta revisão sistemática teve algumas limitações: a primeira e principal limitação é a enorme variabilidade na incidência viral (ou seja, falta de estimativas preliminares do número básico de reprodução [R0] do SARS-CoV-2); a avaliação da eficácia do uso de máscara pode estar diretamente correlacionada à adesão, tempo de uso, tipo de local de exposição, incidência de infecção por COVID-19 no local do estudo, tipo de máscara, distanciamento social e outros fatores. Além disso, os estudos incluídos nesta revisão foram realizados durante a pandemia de COVID-19; no entanto, o R0 de cada estudo provavelmente foi diferente, fato que pode causar resultados bastante diferentes. Além disso, a maioria dos estudos incluídos foi considerada como tendo um sério risco de viés e baixa qualidade de evidência.
Devido à dificuldade em realizar ensaios clínicos randomizados de boa qualidade durante uma pandemia que se espalhou rapidamente pelo mundo, precisávamos trabalhar com as melhores evidências disponíveis.
CONSIDERAÇÕES FINAIS O uso de máscaras mostrou eficácia na prevenção do SARS-CoV-2, independente do tipo de máscara (máscaras cirúrgicas descartáveis, máscaras comuns, inclusive máscaras de tecido, ou máscaras N95). No entanto, a certeza da evidência era baixa.
CONTRIBUIÇÕES DOS AUTORES IF, AS, HAB, AN, ST e WMB: concepção e desenho do estudo. SE e AS: coleta de dados. IF, AS e WB: análises estatísticas e interpretação de dados. WMB e SET: redação do manuscrito. IF, AS, SET, HAB, AN, ST e WMB: revisão crítica e aprovação da versão final do manuscrito.
CONFLITOS DE INTERESSES Nenhum declarado.
REFERÊNCIAS 1.Canini L, Andréoletti L, Ferrari P, D’Angelo R, Blanchon T, Lemaitre M, et al. Surgical mask to prevent influenza transmission in households: a cluster randomized trial. PLoS One. 2010;5(11):e13998. https://doi.org/10.1371/journal.pone.0013998
2.Cowling BJ, Zhou Y, Ip DK, Leung GM, Aiello AE. Face masks to prevent transmission of influenza virus: a systematic review. Epidemiol Infect. 2010;138(4):449-456. https://doi.org/10.1017/S0950268809991658
3.World Health Organization [homepage on the Internet]. Geneva: World Health Organization; c2020 [cited 2020 Apr 8]. Coronavirus disease (COVID-19) advice for the public: When and how to use masks. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public/when-and-how-to-use-masks
4.Centers for Disease Control and Prevention (CDC) [homepage on the Internet]. Atlanta: CDC; c2019 [cited 2020 Apr 8]. Recommendation regarding the use of cloth face coverings, especially in areas of significant community-based transmission. Available: https://www.cdc.gov/coronavirus/2019-ncov/prevent- getting- sick/cloth-facecover html
5.Araujo CM, Guariza-Filho O, Gonçalves FM, Basso IB, Schroder AGD, Cavalcante-Leão BL, et al. Front lines of the COVID-19 pandemic: what is the effectiveness of using personal protective equipment in health service environments?-a systematic review. Int Arch Occup Environ Health. 2022;95(1):7-24. https://doi.org/10.1007/s00420-021-01775-y
6.Coclite D, Napoletano A, Gianola S, Del Monaco A, D’Angelo D, Fauci A, et al. Face Mask Use in the Community for Reducing the Spread of COVID-19: A Systematic Review. Front Med (Lausanne). 2021;7:594269. https://doi.org/10.3389/fmed.2020.594269
7.Chou R, Dana T, Jungbauer R, Weeks C, McDonagh MS. Masks for Prevention of Respiratory Virus Infections, Including SARS-CoV-2, in Health Care and Community Settings : A Living Rapid Review. Ann Intern Med. 2020;173(7):542-555. https://doi.org/10.7326/M20-3213
8.Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71
9.Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. https://doi.org/10.1136/bmj.i4919
10.GRADE Working Group [homepage on the Internet]. c2021 [cited 2021 Aug 1]. GRADE. Available from: https://www.gradeworkinggroup.org/
11.GRADEpro GDT [homepage on the Internet]. Hamilton, Canada: McMaster University and Evidence Prime; c2021. GRADEpro Guideline Development Tool [Software]. Available from: https://www.gradepro.org/
12.Review Manager (RevMan) [Computer Program]. version 5.4. The Cochrane Collaboration; 2020.
13.Chen Y, Tong X, Wang J, Huang W, Yin S, Huang R, et al. High SARS-CoV-2 antibody prevalence among healthcare workers exposed to COVID-19 patients. J Infect. 2020;81(3):420-426. https://doi.org/10.1016/j.jinf.2020.05.067
14.Wang Y, Tian H, Zhang L, Zhang M, Guo D, Wu W, et al. Reduction of secondary transmission of SARS-CoV-2 in households by face mask use, disinfection and social distancing: a cohort study in Beijing, China. BMJ Glob Health. 2020;5(5):e002794. https://doi.org/10.1136/bmjgh-2020-002794
15.Andrejko KL, Pry JM, Myers JF, Fukui N, DeGuzman JL, Openshaw J, et al. Effectiveness of Face Mask or Respirator Use in Indoor Public Settings for Prevention of SARS-CoV-2 Infection - California, February-December 2021. MMWR Morb Mortal Wkly Rep. 2022;71(6):212-216. https://doi.org/10.15585/mmwr.mm7106e1
16.Doung-Ngern P, Suphanchaimat R, Panjangampatthana A, Janekrongtham C, Ruampoom D, Daochaeng N, et al. Case-Control Study of Use of Personal Protective Measures and Risk for SARS-CoV 2 Infection, Thailand. Emerg Infect Dis. 2020;26(11):2607-2616. https://doi.org/10.3201/eid2611.203003
17.Guo X, Wang J, Hu D, Wu L, Gu L, Wang Y. Survey of COVID-19 Disease Among Orthopaedic Surgeons in Wuhan, People’s Republic of China. J Bone Joint Surg Am. 2020;102(10):847-854. https://doi.org/10.2106/JBJS.20.00417
18.Heinzerling A, Stuckey MJ, Scheuer T, Xu K, Perkins KM, Resseger H, et al. Transmission of COVID-19 to Health Care Personnel During Exposures to a Hospitalized Patient - Solano County, California, February 2020. MMWR Morb Mortal Wkly Rep. 2020;69(15):472-476. https://doi.org/10.15585/mmwr.mm6915e5
19.Khalil MM, Alam MM, Arefin MK, Chowdhury MR, Huq MR, Chowdhury JA, et al. Role of Personal Protective Measures in Prevention of COVID-19 Spread Among Physicians in Bangladesh: a Multicenter Cross-Sectional Comparative Study. SN Compr Clin Med. 2020;2(10):1733-1739. https://doi.org/10.1007/s42399-020-00471-1
20.Rebmann T, Loux TM, Arnold LD, Charney R, Horton D, Gomel A. SARS-CoV-2 Transmission to Masked and Unmasked Close Contacts of University Students with COVID-19 - St. Louis, Missouri, January-May 2021. MMWR Morb Mortal Wkly Rep. 2021;70(36):1245-1248. https://doi.org/10.15585/mmwr.mm7036a3
21.Wang X, Pan Z, Cheng Z. Association between 2019-nCoV transmission and N95 respirator use. J Hosp Infect. 2020;105(1):104-105. https://doi.org/10.1016/j.jhin.2020.02.021
22.Xu H, Gan Y, Zheng D, Wu B, Zhu X, Xu C, et al. Relationship Between COVID-19 Infec-tion and Risk Perception, Knowledge, Attitude, and Four Nonpharmaceutical Inter-ventions During the Late Period of the COVID-19 Epidemic in China: Online Cross-Sectional Survey of 8158 Adults. J Med Internet Res. 2020;22(11):e21372. https://doi.org/10.2196/21372














 Read in English
Read in English
 Portuguese PDF
Portuguese PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket