ABSTRACT
Objective: To translate the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire into Brazilian Portuguese and adapt it for use in Brazil. Methods: This methodological study followed internationally recommended guidelines for translation and cross-cultural adaptation. After permission was obtained from the original authors, the process of translation and cross-cultural adaptation began, including translation into Brazilian Portuguese by bilingual translators, synthesis of the translations, back-translation for similarity analysis, revision, and preparation of the final version. A pretest was conducted on 68 medical students. Results: Most of the questionnaire items showed strong content similarity, with minor semantic differences. The content validity index for the questionnaire was 0.882, and Cronbach's alpha coefficients were 0.682, 0.809, and 0.613 for knowledge of tuberculosis, attitudes toward tuberculosis, and preventive behavior toward tuberculosis, respectively. Cronbach's alpha and omega coefficients were a = 0.717, ?1 = 0.673, ?2 = 0.673, and ?3 = 0.520. Conclusions: The process of translation and cross-cultural adaptation of the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire was successful, making the Brazilian Portuguese version of the questionnaire reliable for reproducibility. It can be used in order to collect tuberculosis-related data and support changes in health education curricula.
Keywords:
Tuberculosis; Cross-cultural comparison; Attitude; Behavior.
INTRODUCTION Despite efforts by the WHO and many countries to eliminate tuberculosis, incidence and mortality rates have declined slowly, tuberculosis remaining a major global health concern. This situation has been worsened by COVID-19 and recent armed conflicts, creating a pressing global tuberculosis crisis. Well-structured, effective, and multisectoral responses are essential in order to meet eradication targets.(1)
In Brazil, the National Plan to End Tuberculosis as a Public Health Problem, issued in 2017, has not been able to prevent more than 80,000 new cases and approximately 5,000 deaths annually. Brazil ranks alongside nations such as Bangladesh and Zambia,(2) reflecting gaps in tuberculosis prevention, diagnosis, treatment, and research investments.(3)
Between 2015 and 2023, tuberculosis cases increased, particularly among vulnerable groups. From 2022 to 2023, tuberculosis cases among health care workers also rose.(2) Recognizing and preventing tuberculosis is crucial not only for patient care but also for health care professionals.
Assessing knowledge, attitudes, and behaviors regarding tuberculosis among health students can enhance disease recognition, improve patient care, and foster empathy toward infected individuals. Findings can inform policy decisions and curriculum enhancements in health education, which remains an area requiring further research.(4-7)
The WHO developed the Knowledge, Attitudes, and Practices (KAP) questionnaire in the 1950s to assess various health issues. The tuberculosis-specific version, available since 2008, provides guidance on adapting the questionnaire to different social contexts.(8) However, although the KAP questionnaire is effective for general knowledge assessment, it has limitations in evaluating tuberculosis-related practices and attitudes.(9)
The Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire, developed by Yun Choi and Geum Hee Jeong and published in English in 2018,(10) was initially designed to assess knowledge of, attitudes toward, and preventive behaviors toward tuberculosis among Korean army soldiers. The questionnaire integrates KAP questionnaire components, features clear and concise statements, and is suitable for international studies. However, it has yet to be translated and adapted for use in Brazil.
The objective of the present study was to translate the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire into Brazilian Portuguese and adapt it for use among health students in Brazil.
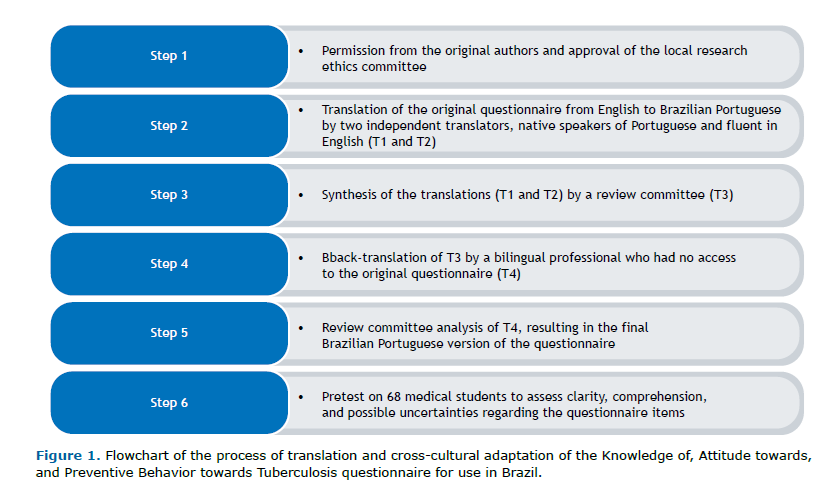
METHODS This study is a methodological investigation of translating the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire into Brazilian Portuguese and adapting it for use in health students in Brazil. The study followed methodological guidelines from Beaton et al. and Fortes & Araújo, who proposed that self-report measures be cross-culturally adapted in accordance with international recommendations, following the steps of preparation, translation, reconciliation of translations, back-translation, revision, and pretesting.(11,12)
The original scale was based on an examination tool by the Korean Centers for Disease Control and Prevention(10) and is multidimensional, measuring knowledge, attitudes, and preventive behavior related to tuberculosis, with original Cronbach's alpha coefficients of 0.87, 0.83, and 0.82, respectively.(12) To measure tuberculosis knowledge, 20 items (six of which are formulated in reverse) offer three response options (yes, no, and I don't know)(10) with binomial correction (correct/incorrect). The sections measuring attitudes and behavior each contain 15 items with positive statements scored on four-point Likert scales, higher scores translating to better attitudes and more appropriate behaviors toward tuberculosis. The tool offers the advantage of being evaluated by items or subcategories for each section.
The adaptation process began with permission from the original authors. Ethical considerations were adhered to, and approval was obtained from the Research Ethics Committee of the São Paulo State University School of Medicine at Botucatu (Ruling nos. 5.278.736 and 5.453.561), in accordance with Brazilian National Health Council Resolution nos. 510/2016 and 466/2012.
The original questionnaire was independently translated into Brazilian Portuguese by two Brazilians who were fluent in English, one of whom is in the field of health sciences and one of whom is in the field of biological sciences. The translators were identified as translator 1 and translator 2, producing two independent translations (T1 and T2). For the synthesis of the translations, a review committee was formed, including medical and nursing professionals, as well as a researcher experienced in translating and culturally adapting self-report measures. All committee members have a doctoral degree and knowledge of English and Brazilian Portuguese. The committee held meetings to compare translations and discuss until a consensus version was agreed upon (T3).
The evaluation considered semantic equivalence, idiomatic equivalence, cultural equivalence, and conceptual equivalence. The resulting version was then back-translated into English by an independent professional who is fluent in Portuguese and English, and who had no medical training, being unaware of the original English-language version of the questionnaire. This process resulted in a back-translation (T4), which was compared with the original for similarity analysis.
To better assess the internal consistency of the questionnaire, the committee expanded the four-point Likert scales to six points in the attitudes and behavior domains, with a minimum score of 15 and a maximum score of 90.
For calculation of the content validity index, each item was scored on a Likert scale from 1 to 4 on the basis of the feasibility of translation to the Brazilian context.(13) The content validity index for the entire questionnaire was calculated as the arithmetic mean of the item scores, with 100% as the approval parameter.(14)
A pilot test was conducted on 68 medical students at a public university in Brazil. After completing the questionnaire, student judges evaluated clarity, comprehension, and possible uncertainties regarding the items, being given an opportunity to suggest improvements. On the basis of the mean of positive scores, the minimum acceptable value was set at 0.80. The entire process of translation and cross-cultural adaptation is shown in Figure 1.
To assess internal consistency, the Kuder-Richardson formula 20 was used for knowledge-related items, whereas Cronbach's alpha and Omega coefficients were applied with values between 0.60 and 0.95 being considered acceptable.(15-17) Additionally, item-total correlation was analyzed, with correlations greater than 0.20 suggesting good correlation.(18,19)
RESULTS The process of translation and adaptation of the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire occurred between May of 2023 and March of 2024. Of the 50 questionnaire items, 49 showed strong content similarity, with only minor semantic differences.
In the process of translating the 50 items that constitute the questionnaire, similarities prevailed in 49 (98%) of the items regarding content, with few semantic differences. Only one item had exact similarity.
For the consensus version (T3), T1 and T2 were adapted to the Brazilian culture and context, in accordance with the WHO KAP guidelines.(8) The review committee standardized the items by using the first-person pronoun "I". The committee opted for terms that are more commonly used by patients ("phlegm," "tiredness," and "fever" instead of "expectoration/sputum," "fatigue," and "sweating"), as well as culturally appropriate terms ("glasses and cutlery" instead of "bowls").
Adjustments related to the medical context were necessary because, according to the current literature, smoking is a relevant factor for greater susceptibility to tuberculosis, regardless of frequency (item 7). For the item referring to nocturnal fever, the committee opted for "nocturnal period" rather than "at dusk," considering that patients do not always correctly identify specific times (item 11).
To ensure clarity, the committee maintained the term "medicines" in some items to avoid repetition while preserving comprehension. Adjustments for terms commonly accepted in Brazil were necessary, such as in items 23, 24, 25, and 28 ("I think" and "I believe").
In the back-translation (T4), there were differences from the original because of the need to make adjustments; however, there were no conceptual errors or inconsistencies detrimental to the evaluation. The back-translation reproduced the same ideas as did the items in the original version, passing the validity checks and having no potential errors. The content validity index for the questionnaire was 0.95 in the first evaluation and 1.00 in the second, expert consensus being achieved for all items.
A pretest was conducted in March of 2024. Most of the students to whom the questionnaire was administered were < 25 years of age (80.9%), female (57.4%), single (98.5%), and nonsmokers (91.2%). Only 7.4% of the respondents reported tuberculosis cases in their families. The mean knowledge score was 10.51, with 79% (n = 54) failing to answer 70% of questions correctly. In the attitudes domain, the mean total score was 72.3 [IQR, 20-90], being = 4.82 per item, with the mean score being lowest (2.34) for item 26. For the behavior domain, the mean total score was 61.1 [IQR, 38-87], being 4.08 per item, with the mean scores being lowest (1.57, 1.56, and 1.46) for items 42, 43, and 44, respectively.
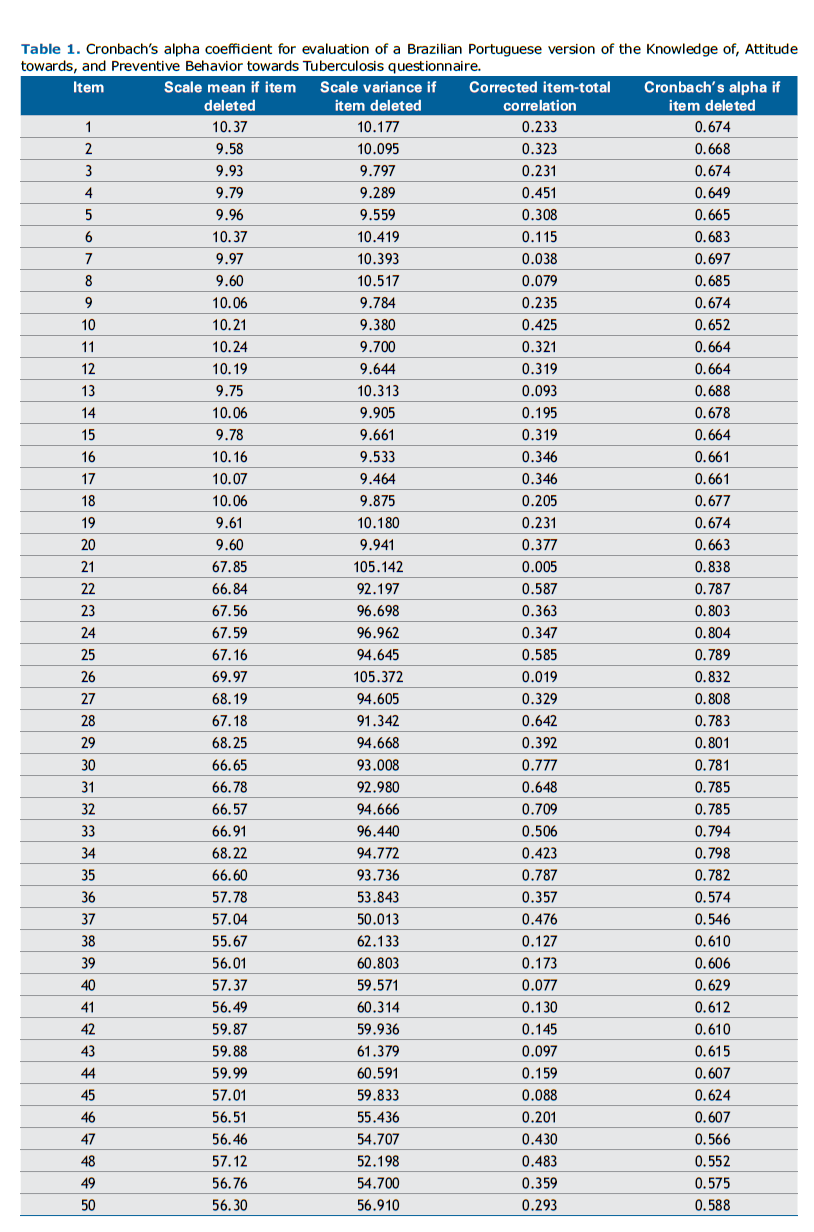
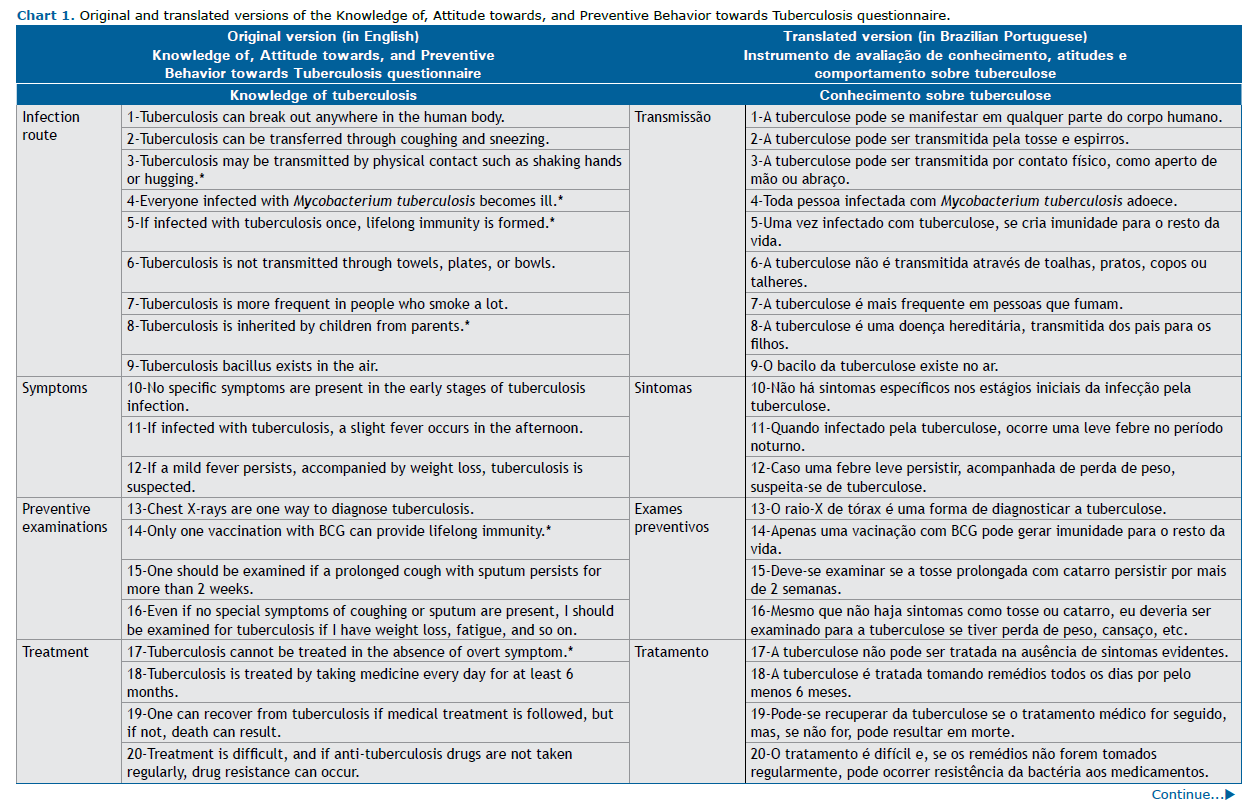
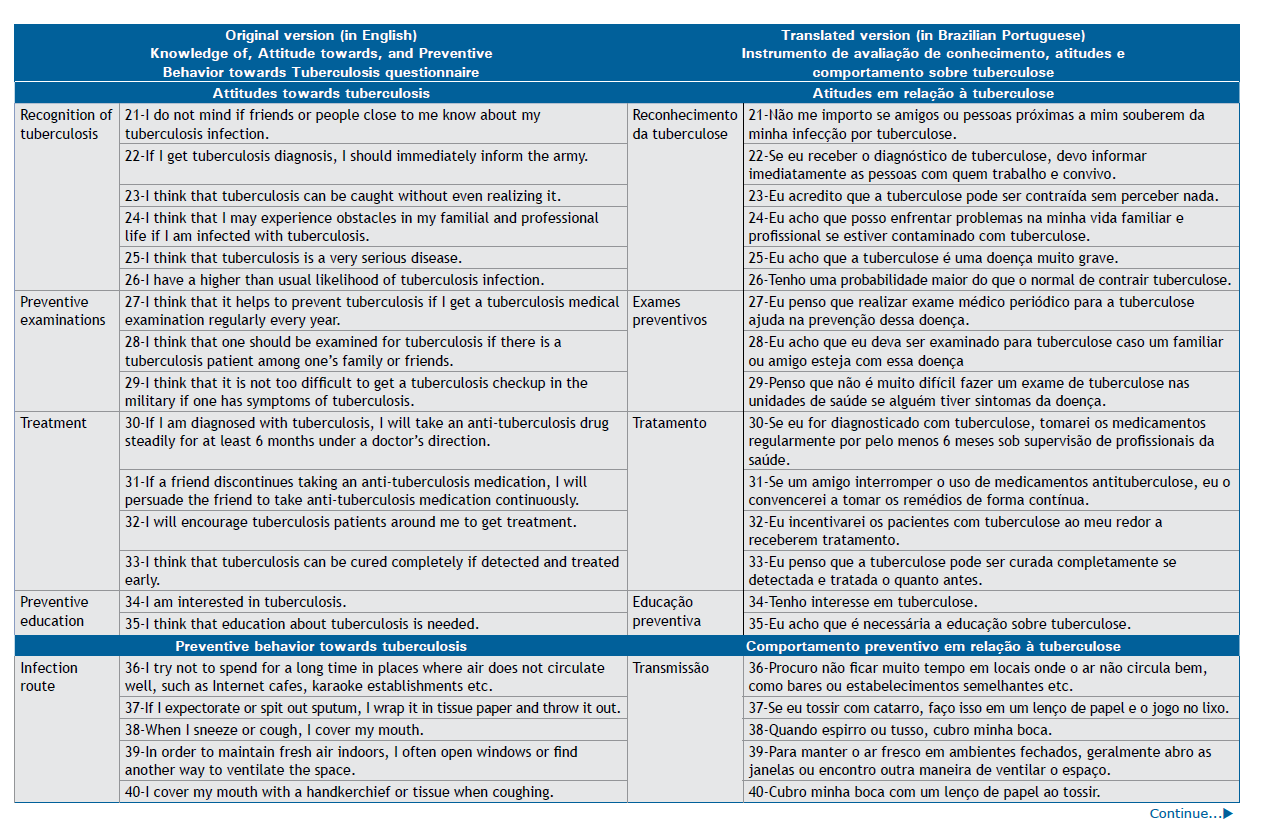
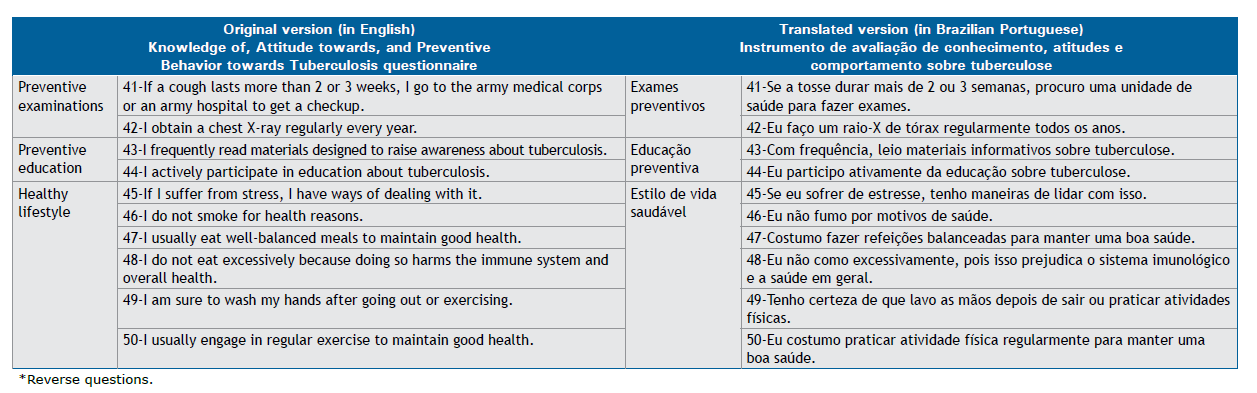
In the evaluation of the questionnaire, the mean coefficient calculated for clarity, comprehension, and uncertainty was 0.882. In the analysis of the internal consistency of the questionnaire, Cronbach's alpha coefficients were 0.682 for knowledge of tuberculosis, 0.809 for attitudes toward tuberculosis, and 0.613 for preventive behavior toward tuberculosis (Table 1). With regard to Cronbach's alpha and McDonald's omega coefficients, the results were as follows: a = 0.717 and ?1 = 0.673; ?2 = 0.673; and ?3 = 0.520 for knowledge of tuberculosis, attitudes toward tuberculosis, and preventive behavior toward tuberculosis, respectively. The highest item-total correlations were obtained in the attitudes domain (Table 1). Chart 1 shows the original English-language version of the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire and the Brazilian Portuguese version of the questionnaire.
DISCUSSION The present study described the process of developing a Brazilian Portuguese version of the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire for undergraduate health students, following the methodological steps recommended in the literature. The translated questionnaire achieved semantic, idiomatic, conceptual, and cultural equivalence, with adequate comprehension by the target population and good internal consistency.
The use of international scales facilitates comparisons of studies across countries, expanding opportunities for successful interventions. However, cross-cultural adaptation of instruments requires a meticulous process involving multiple stages that address both textual and technical aspects.(20) This demands methodological rigor to maintain the reliability and validity of the original instrument.(21)
The Consensus-based Standards for the Selection of Health Measurement Instruments initiative recommends that translated versions of assessment tools undergo review by a committee of experts and pretesting to improve the selection of instruments for measuring outcomes in research and clinical practice, thus contributing to the development of assessment tools that are more appropriate.(22)
Although the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire is a comprehensive, 50-item questionnaire, its concise, objective, and easy-to-understand sentences facilitated the process of translating it into the target language. Backward translation ensured equivalence between the translations and the original English-language questionnaire.
In making necessary adaptations to the local culture, the expert committee compared translations without major controversies or disagreements among members, consistently considering scientific evidence on the subject(23) and focusing on effective communication by selecting the terms that are most commonly used by patients and laypeople in general,(24) aiming for an approach aligned with the Brazilian reality. The clear and detailed completion guidelines appear to have been fundamental to data collection. Similar results can be found in the literature, highlighting the importance of pretesting, given that this stage can identify potential difficulties in completing, applying, or understanding the items.(25)
Because the Knowledge of, Attitude towards, and Preventive Behavior towards Tuberculosis questionnaire was originally developed with the use of simple language, our study sought to expand its use. We examined each item in detail and its appropriateness within any scope of practice and determined that no items needed to be excluded. The pretest results indicated that the participants understood the questionnaire well.
Although Cronbach's alpha remains the most commonly used reliability index in research, several other aspects of test capability should be considered, including validity evidence, intercultural fairness, and practicality. The limitations of Cronbach's alpha have been discussed elsewhere,(17) with better alternatives including omega coefficients, which offers advantages for applied research in which items differ in quality or have skewed distributions. Omega coefficients can extend the usefulness of alpha coefficients in estimating the reliability of internal consistency scores on a multidimensional scale with smaller samples,(17) such as the one evaluated in the present study.
In general, most of the students in our sample did not have adequate knowledge of tuberculosis at the time of questionnaire administration, despite their attitudes and behaviors being considered positive. Our results regarding tuberculosis knowledge are similar to those obtained in Korea, where the instrument was developed (11.64; 58.2%), with low recognition of populations more vulnerable to tuberculosis, as well as low scores on questions related to behavior, especially those concerning examinations and preventive education.(10)
In a scenario in which tuberculosis continues to be a neglected disease, translating and adapting a tuberculosis questionnaire fulfills the objective of providing an instrument that can enable comparisons and identification of gaps in teaching, as well as the implementation of policies to ensure that tuberculosis becomes an integral part of any educational curriculum for health professionals. Given the widespread need to promote public policies that guarantee continuous improvement of care and effectiveness of measures to control and prevent tuberculosis, it is essential to include tuberculosis education in the curricula of future health professionals.(26)
The absence of experts from other regions of the country in the evaluation may have been a limiting factor in the present study, given that Brazil is a large, culturally diverse country. Future studies should focus on the application of the final version of the questionnaire, its psychometric validation, and its use in other health professionals .
The recommendation to use internationally standardized instruments is aimed at improving research quality and enabling more reliable comparisons between countries and regions. Our translation and cross-cultural adaptation of a questionnaire for assessing knowledge, attitudes, and behaviors regarding tuberculosis offers an important resource for researchers in Brazil by providing a version translated and revised by an expert committee, and subjected to pretesting and statistical analysis in accordance with international guidelines. The use of the translated questionnaire can contribute to collecting information on tuberculosis and support changes in health education curricula.
AUTHOR CONTRIBUTIONS RMBC and SPFF: study conception and design; and drafting of the manuscript. RMBC, SPFF, RCA, and HRCN: analysis and interpretation of data. RMBC, SPFF, RCA, HRCN, and SAML: revision of the manuscript. All authors approved the final version of the manuscript.
CONFLICTS OF INTEREST None declared.
REFERENCES 1. Villar-Hernández R, Ghodousi A, Konstantynovska O, Duarte R, Lange C, Raviglione M. Tuberculosis: current challenges and beyond [published correction appears in Breathe (Sheff). 2023;19(2):225166. doi: 10.1183/20734735.5166-2022.]. Breathe (Sheff). 2023;19(1):220166. https://doi.org/10.1183/20734735.0166-2022
2. Brasil. Ministério da Saúde. Boletim Epidemiológico Secretaria de Vigilância em Saúde. Número Especial. Mar 2023. ISSN 9352-7864. Available from: https://www.gov.br/saude/pt-br/centrais-de-conteudo/publicacoes/boletins/epidemiologicos/especiais/2023/boletim-epidemiologico-de-tuberculose-numero-especial-mar.2023#:~:text=Por%20conseguinte%2C%20no%20primeiro%20ano,a%20cada%20100%20mil%20hab
3. Maciel EL, Golub JE, Silva JRLE, Chaisson RE. Tuberculosis: a deadly and neglected disease in the COVID-19 era. J Bras Pneumol. 2022;48(3):e20220056. https://doi.org/10.36416/1806-3756/e20220056
4. Matarazo JGA, Kito BK, Boni FNG, Merighi DGS, Lordelo ASB, Silva AF, et al. Conhecimento, atitudes e práticas sobre a tuberculose de estudantes universitários da área da saúde [Article in Portuguese]. Braz J Infect Dis. 2022:26(2):102543. https://doi.org/10.1016/j.bjid.2022.102543.
5. Paschoal GS, Souza GS, Pereira M, Carvalho LPF. Tuberculose: os futuros profissionais de saúde são preparados para o atendimento adequado do paciente? Int J Educ Health. 2018;2(1):73-81. https://doi.org/10.17267/2594-7907ijhe.v2i1.2045
6. Carvalho CF, Ponce MAZ, Silva-Sobrinho RA, Mendez RDR, Santos MA, Santos EM, Wysocki AD. Tuberculosis: knowledge among nursing undergraduate students. Rev Bras Enferm. 2019;72(5):1279-1287. https://doi.org/10.1590/0034-7167-2018-0384
7. Poletto PR, Jurdi APS. A experiência de revisão das matrizes curriculares em um projeto pedagógico inovador: caminhos para fortalecer a educação interprofissional em Saúde [article in Portuguese]. Interface (Botucatu). 2018;22(Suppl. 22):1777-86. https://doi.org/10.1590/1807-57622017.0819
8. World Health Organization (WHO) [homepage on the Internet]. Geneva: WHO [cited 2024 Dec 1]. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys. 2008. WHO/HTM/STB/2008.46. Available from: https://iris.who.int/bitstream/handle/10665/43790/9789241596176_eng.pdf
9. Ferreira Júnior S, Oliveira HB, Marin-Léon L. Knowledge, attitudes and practices on tuberculosis in prisons and public health services [Article in Portuguese]. Rev Bras Epidemiol. 2013;16(1):100-113. https://doi.org/10.1590/S1415-790X2013000100010
10. Choi Y, Jeong GH. Army Soldiers' Knowledge of, Attitude Towards, and Preventive Behavior Towards Tuberculosis in Korea. Osong Public Health Res Perspect. 2018; 9(5):269-277. https://doi.org/10.24171/j.phrp.2018.9.5.09
11. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the Process of Cross-Cultural Adaptation of Self-Report Measures. Spine (Phila Pa 1976). 2000;25(24):3186-3191. https://doi.org/10.1097/00007632-200012150-00014
12. Fortes CPDD, Araújo APQC. Check list for healthcare questionnaires cross-cultural translation and adaptation [Article in Portuguese]. Cad Saude Colet. 2019;27(2):202-9. https://doi.org/10.1590/1414-462X201900020002
13. Korea Centers for Diseases Control and Prevention (KDCA) [homepage on the Internet]. KDCA: Cheongju [cited 2024 Dec 1]. National guideline for tuberculosis control 2013. Available from: https://www.cdc.go.kr/
14. 14.Alexandre NM, Coluci MZ. Content validity in the development and adaptation processes of measurement instruments [Article in Portuguese]. Cien Saude Colet. 2011;16(7):3061-3068. https://doi.org/10.1590/S1413-81232011000800006
15. Hajjar STE. Statistical analysis: internal-consistency reliability and construct validity. Int J Quant Qual Res Methods 2018;6(1):46-57. https://doi.org/10.37745/ijqqrm.13
16. Trizano-Hermosilla I, Alvarado JM. Best Alternatives to Cronbach's Alpha Reliability in Realistic Conditions: Congeneric and Asymmetrical Measurements. Front Psychol. 2016;7:769. https://doi.org/10.3389/fpsyg.2016.00769
17. Kalkbrenner MT. Alpha, Omega, and H Internal Consistency Reliability Estimates: Reviewing These Options and When to Use Them. Counsel Outcome Res Evaluat. 2023;14(1):77-88. https://doi.org/10.1080/21501378.2021.1940118
18. Matta SR, Azeredo TB, Luiza VL. Internal consistency and interrater reliability of the Brazilian version of Martín-Bayarre-Grau (MBG) adherence scale. Braz J Pharm Sci. 2016;52(4):795-799. https://doi.org/10.1590/S1984-82502016000400025
19. Zijlmans EAO, Tijmstra J, van der Ark LA, Sijtsma K. Item-Score Reliability as a Selection Tool in Test Construction. Front Psychol. 2019;9:2298. https://doi.org/10.3389/fpsyg.2018.02298
20. Nora CRD, Zoboli E, Vieira MM. Validação por peritos: importância na tradução e adaptação de instrumentos [Article in Portuguese]. Rev Gauch Enferm. 2017;38(3):e64851. https://doi.org/10.1590/1983-1447.2017.03.64851
21. Lino CRM, Brüggemann OM, Souza ML, Barbosa SFF, Santos EKA. The cross-cultural adaptation of research instruments, conducted by nurses in Brazil: an integrative review. Text Context Enferm. 2017;26(4):e1730017. https://doi.org/10.1590/0104-07072017001730017
22. Mokkink LB, Prinsen CA, Bouter LM, Vet HC, Terwee CB. The COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) and how to select an outcome measurement instrument. Braz J Phys Ther. 2016;20(2):105-113. https://doi.org/10.1590/bjpt-rbf.2014.0143
23. Faria L, Oliveira-Lima JA, Almeida-Filho N. Medicina baseada em evidências: breve aporte histórico sobre marcos conceituais e objetivos práticos do cuidado. Hist Cienc Saude Manguinhos. 2021;28(1):59-78. https://doi.org/10.1590/S0104-59702021000100004
24. Campos CFC, Fígaro R. A Relação Médico-Paciente vista sob o Olhar da Comunicação e Trabalho. Rev Bras Med Fam Comum. 2021;16(43):2352. https://doi.org/10.5712/rbmfc16(43)2352
25. Lima GA, Lima FET, Florencio S de SG, Fontenele MGM, Ventura MWS, Barbosa LP, et al. Translation and cross-cultural adaptation of the Parental Perception on Antibiotics Scale: Brazilian version. Acta Paul Enferm 2023;36:eAPE03292. https://doi.org/10.37689/acta-ape/2023AO03292
26. Picanço L, Dutra RP, Saes MO. Temporal trend in the evaluation of adequate management for diagnosis and treatment of tuberculosis in primary health care in Brazil (2012-2018). Cad Saude Publica. 2024;40(3):e00087723. https://doi.org/10.1590/0102-311XPT087723





 English PDF
English PDF
 Print
Print
 Send this article by email
Send this article by email
 How to cite this article
How to cite this article
 Submit a comment
Submit a comment
 Mendeley
Mendeley
 Pocket
Pocket






